The authors present a case report of dens in dente in an upper molar, in which endodontic treatment was impossible due to its location.
Key Words: dens in dente, dens invaginatus, therapy.
Introduction
Dens in dente is an anomaly of development resulting from deepening or invagination of the enamel organ into the dental papilla, which begins at the crown and often extends to the root, before the calcification of the dental tissues.
The first observation of dens in dente dates back lo 1856 (De Smit and Demaut, 1982). This anomaly is also known as dens invaginatus, dilated odontome and gestant anomaly. According to Pécora et al. (1990), the varied nomenclature occurs probably due to the lack of consensus in relation to the cause of this alteration and the various names reflect the different opinions as to its etiology.
Hovland (1977) calculated the incidence of dens in dente to be 0.04 to 10.00%, occurring in any tooth but with a greater frequency in the permanent upper lateral incisors. Cases of bilateral occurrence have been reported (Swanson and McCarthy, 1947; Grossman, 1976; Burton et al., 1980).
Dens in dente is classified into 3 types, depending on the depth of invagination. Type I, the invagination ends in a blind sac, limited to the dental crown. Type II, the invagination extends to the amelocemental junction, also ending in a blind sac. Type III, the invagination extends to the interior of the root, providing an opening to the periodontium, sometimes presenting another foramen in the apical region of the tooth (Oehlers, 1957).
Radiographically, dens in dente shows a radiopaque invagination similar in density to dental enamel (Goaz and While, 1987).
Maisto (1973), Tagger (1977), Cole et al. (1978), Eldeeb (1984), Pécora et al. (1987, 1990), and Vajrabhaya (1989) report cases of dens in dentetreated with conventional endodontic methods. However, Fergunson et al. (1980), Schindler and Walker (1983), and Pécora et al. (1987, 1990) describe special endodontic techniques capable of inducing an apexification in Oehlers Type II dens in dente. Weine (1982) and Leonardo et al. (1982) report the endodontic treatment of dens in dente as being a difficult operation, preferring surgical treatment with retrograde filling.
Case Report
A 26 year old, white, female patient was referred to our clinic with pain in the upper left region. Clinical examination showed edema of the vestibular cul-de-sac region, at the level of the second upper left molar, which did not respond to thermal tests (heat and cold) but responded positively to palpation and percussion.
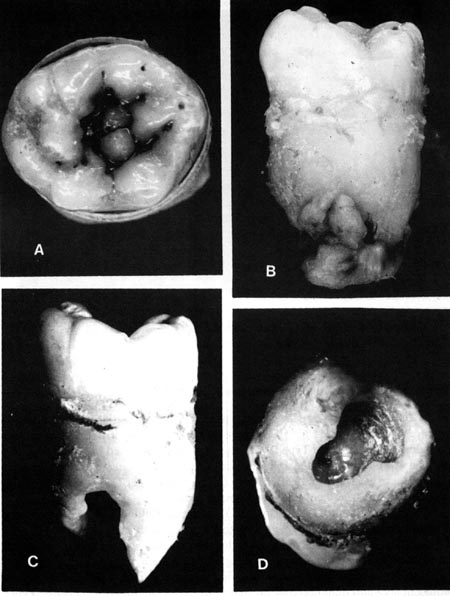
An x-ray showed the presence of Type III (Oehlers, 1957) dens in denteof the second upper left molar with an apical radiolucent area (Figure 1).
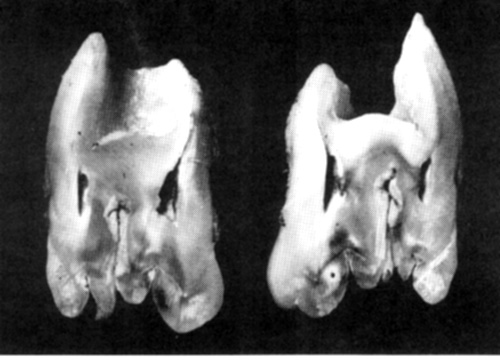
Due to the localization of the tooth and the impossibility of endodontic root canal treatment, complemented by the retrograde filling of the apical opening, the treatment of choice was extraction (Figures 2 and 3).
Discussion
The presence of dens in dente is more common in the lateral upper incisors, being rare in molars. Types I and II (Oehlers, 1957) dens in dente do not present problems in endodontic treatment. In Type II, the invagination is restricted to the interior of the root canal without reaching the apical region of the canal, ending in a single foramen.
Pécora et al. (1987, 1900), Maisto (1973) and Tagger (1977) present methods for the endodontic treatment of Type II dens in dente.
Hata and Toda (1987), Bolanos (1988) and Kulild (1989) recommend the endodontic treatment of dens in dente in anterior upper teeth, even in Type III (Oehiers, 1957) cases. In these cases, conventional endodontic treatment in the area of invagination must be complemented by retrograde filling of the foramen of the principal canal.
In the case reported here, the first upper left molar presented an apical radiolucent area and pulp necrosis, probably due to the fact that dens in dente, Types II and III (Oehlers, 1957), permits the penetration of irritants into the interior pulp tissue once the invagination establishes this communication with the buccal cavity. Contamination can also occur by communication with the pulp through the cul-de-sac of the invagination causing tissue necrosis.
The current literature does not present solutions for the treatment of Type III dens in dente in molars which will only be possible when the retrograde filling of the root canal is viable.
References
Bolanos OR, Martell B, Morse DR: A unique approach to the treatment of a tooth with dens invaginatus. J Endodont 14: 315-318, 1988
Burton JD, Saffos RO, Scheffer RB: Multiple bilateral dens in dente as a factor in the etiology of multiple periapical lesions. Oral Surg 49: 496-499,1980
Cole GM, Taintor JF, James GA: Endodontic therapy of a dilated dens invaginatus. J Endodont 4: 89-90, 1978
De Smit A, Demaut L: Nonsurgical endodontic treatment of invaginatus teeth. J Endodont 8: 506-511, 1982
Eldeeb ME: Nonsurgical endodontic therapy of a dens invaginatus. J Endodont 10: 107-109, 1984
Fergunson FS, Friedman S, Frazzetto V: Successful apexification technique in an immature tooth with dens in dente. Oral Surg 49: 356-359, 1980
Goaz PW, White SC: Oral radiology. Principles and interpretation. Mosby, St Louis 1987
Grossman LI: Endodontia prática. Guanabara-Koogan, Rio de Janeiro 1976
Hata I, Toda T: Treatment of dens invaginatus by endodontic treatment of dens invaginatus, apicocuretage and retro-filling: a case report. J Endodont 13:469-472, 1987
Hovland EJ: Nonrecognition and subsequent endodontic treatment of dens invaginatus. J Endodont 3: 360-361,1977
Kulild JC, Weller N: Treatment considerations in dens invaginatus. J Endodont 15: 381-384, 1989
Leonardo RM, Leal, JM, Simões AP: Endodontia: Tratamento dos canais radiculares. Panamericana, São Paulo 1982
Maisto OA: Endodontia. Mundi, Buenos Aires 1973
Oehlers FA: Dens invaginatus: Variation of the invagination process and associated anterior crown forms. Oral Surg 10: 1204-1218, 1957
Pécora JD, Costa WF, Macchetti DD: Caso clínico: Dens in dente. Rev Odont USP 1: 46-49, 1987
Pécora JD, Vansan LP, Gariba Silva R, Aiello JSS: Dens invaginatus: Tratamento endodôntico em uma sessão. Rev Ass Paul Cirurg Dent (in press) 1990
Swanson WF, McCarthy FM: Bilateral dens in dente. J Dent Res 26: 167-171, 1947
Schindler WC, Walker WA: Continued root development after apexification of an immature tooth with dens invaginatus. J Endodont 9: 430-433,1983
Tagger M: Nonsurgical endodontic therapy of tooth invagination. Oral Surg 43: 124-129, 1977
Vajrabhaya L: Nonsurgical endodontic treatment of tooth with double dens in dente.J Endodont 15: 323-327, 1989
Weine FS: Endodontic therapy. Mosby, St. Louis 1982
{kind=link}
{kind=link}
{kind=link}